
Table Of Contents
- Options for Stage II Melanoma: Making the Decision That’s Right For You
- What is Stage II melanoma?
- Is Stage II melanoma at high risk for coming back (recurring)?
- It is true that Stage II melanoma can have a worse prognosis than Stage III melanoma?
- How can I lower the risk of Stage II melanoma coming back? What adjuvant drugs are used?
- What are the side effects of adjuvant therapy?
- How is adjuvant therapy given?
- How do you weigh the benefits and risks of adjuvant therapy vs active surveillance?
- What do you tell patients who have Stage IIA melanoma and are worried about their risk for recurrence?
Dr. Geoffrey Lim: Before the FDA approval of adjuvant therapy for Stage II disease, we had nothing to offer these patients to mitigate the risk of their melanoma coming back. These are patients who do not have metastatic disease. Clinicians are used to having these adjuvant therapy conversations with patients with metastatic lymph node disease. How do you discuss the option of adjuvant therapy for patients with Stage IIB and IIC disease in terms of mitigating their risk for recurrence?
Dr. Jason Luke: A strange thing about adjuvant therapy, which often stretches people’s usual thought process, is that you’ll never know if the treatment worked after the surgery. You’ll only know if it didn’t work. Because if it works, the melanoma will never come back, but the melanoma might never have come back anyway. So how do you know whether the disease would not have come back anyway or if the adjuvant therapy prevented it from coming back?
Also, right now, we don’t know whether adjuvant therapy is better than waiting for metastatic disease and then providing treatment. We don’t know whether adjuvant therapy helps people live longer than they would if we just treated them when the disease returned. Adjuvant therapy clearly reduces recurrence, which I believe is a good thing in and of itself because that alleviates psychological stress. But we don’t know yet whether or not that’s going to increase the survival rate for the average patient.
Understanding what risk reduction with adjuvant therapy means for you
Dr. Jason Luke: How different people accept information about their risk of recurrence and what it means to them can be very different. We will go through the actual risk recurrence data below, but it ultimately comes down to an individual person’s priorities and risk tolerance. You can imagine scenarios where somebody says, “Well, I’m already sick of dealing with my melanoma and I have other problems that might be more pressing right now, and I’m not even worried about five years from now.” For that person, active surveillance might make sense. Or, you may have somebody else who says, “This sounds like a really, really big deal, and I want to do whatever is possible to try to mitigate that risk.” That person may be willing to accept the risk of side effects to gain potential benefit from adjuvant therapy.
So, what we talk about is what do these numbers mean? And so, there’s this percent risk that the melanoma could come back. This is called the baseline risk of recurrence. What does that number mean to you? Because people do often have a gut sense of this. They think, oh, that sounds like a lot, or that doesn’t sound like a lot. And that can give you a real strong initial sense of shared decision making about what’s going to be the right decision for them.
We then start to talk to them about adjuvant therapy. Here’s the treatment option that we might have to offer in that case. At this time, immunotherapy that was approved for more advanced melanoma, as we mentioned before, has been studied in Stage II melanoma. And very similar to what we see in other higher stages, immunotherapy reduces the risk of the melanoma coming back by approximately 35%, 40%, somewhere around there.
We try to make sure these discussions are straightforward for people. Another important discussion point is the concept of relative versus absolute risk reduction. If we quote a 30% or 40% risk reduction, you have to take that initial risk recurrence number (28%-45% for Stage IIB and IIC melanoma) and reduce it by 30% to 40%. Then you have to clarify that even with adjuvant treatment, the risk of recurrence doesn’t entirely go away.
To be more granular, if we quoted you a recurrence risk of 30% and then said that we’re reducing that by 30%, that’s only about 9% off the 30% (Graphic). So, then you get to a 21% chance of recurrence. So now the question becomes is a 30% chance of recurrence without adjuvant treatment versus a 21% chance of recurrence with treatment useful to you? And how do you balance that with the risk of side effects, etc?
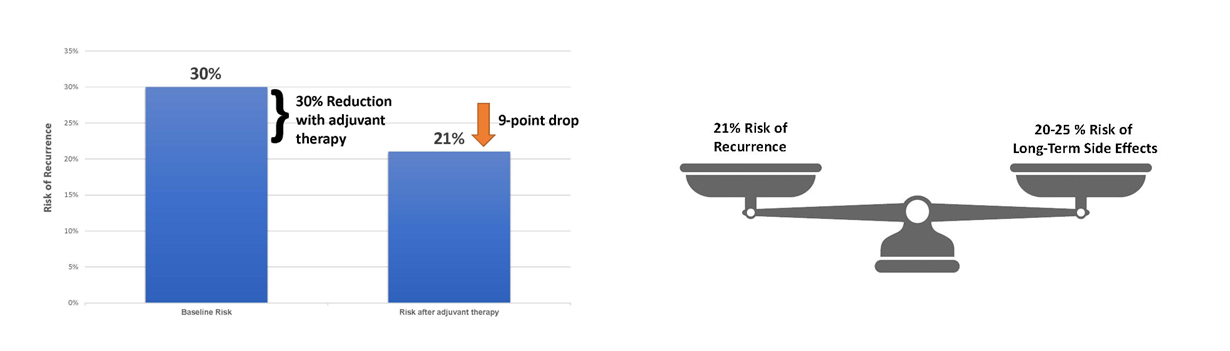
Graphic. Representation of the potential calculation of risk reduction and weighing vs side effects of immunotherapy used in the Stage IIB melanoma adjuvant setting.
Dr. Geoffrey Lim: But there’s other aspects of drug treatment to consider such as how well tolerated are these medicines? And for the patient that is really thinking about pushing the go button here, what types of things do you lay out to consider that may actually sway them the other way, whether it be toxicities or otherwise?
Weighing the risks
Dr. Jason Luke: These drugs can then cause a fairly significant impact on people’s quality of life. If they experience certain side effects (like low thyroid hormone), then they may have to take a medicine for the rest of their life. When you start talking about a permanent side effect, that’s a big consideration. So, this is where that gut check sense from the patient really makes a big difference. So, when you tell them their risk, do they think, “Oh my gosh, that’s huge!” Or do they think, “Well, I’m not so sure, because often where we land is somewhere where we have an approximately similar risk of a long-term problem versus the amount of benefit with risk reduction of the melanoma coming back.” (See Graphic) The reality is that the risks for side effects may be a little higher in healthy patients receiving adjuvant therapy vs patients with metastatic melanoma. We think this may be because patients with advanced cancer have had their immune systems beaten down by the cancer. In the earlier stages of melanoma, the immune system hasn’t been beaten down, so it is more likely to get revved up and may cause collateral damage to organs. Obviously, we want to be in a place where there’s more risk reduction of melanoma than potential side effects, but sometimes we aren’t that far off, quite frankly.
So, the question then is how does an individual patient consider that? Do they think, “I’m going for all the risk reduction because I don’t want the melanoma to come back,” or is their perspective, “Well, I don’t know, maybe it’s not that high risk, and I really don’t want the side effects.” And that, in the end, often is the consideration. And that’s where I think not rushing to a decision is really, really important in terms of taking the time to weigh risks and benefits. Because if you get one of the side effects, you’re not going to “un-get” it, right? But similarly, if the melanoma comes back, you’re not going to “un-have it” either. And so that’s really the decision point for patients.
I try to keep this conversation away from the, “I’m just scared, I’m going to do this,” to a real consideration of risks and benefits. We have to try to help patients stay there and think, because I think it’s very easy to just defer to, well, “I’m scared, I’ll take whatever you tell me.”
Shared decision making
Dr. Jason Luke: When we think about making decisions for post-surgical adjuvant treatment, we often don’t make a decision the first time we talk through everything with the patient because it can be overwhelming to think through all of this. Many people have never thought about whether or not a 20% versus 30% risk is something that’s meaningful to them. So, we really try to share the information, help people get that gut sense of things, and then often maybe take a little time to think about it because we’re not in a big rush. We can chat on the phone; we can see someone back in a week or two, and we can talk through it again.
And I fully understand that many patients start to get a little lost as we start jogging through these numbers. And that’s where having support from a family member who’s either taking notes or is just listening on their own can be very, very helpful.
Dr. Geoffrey Lim: And of course, you mentioned a good point about how we don’t make decisions in a vacuum in the clinic. Often times it takes time to digest, bring family members into the discussion, meditate on it, whatever you need to do.
Dr. Jason Luke: This is really a joint decision-making progress. There are a lot of numbers and percentages that get thrown all around, but in the end, we want to do something that you as a patient or that you with your family feel the most confident in. And that shouldn’t necessarily be the doctor just telling you what to do. You need to absorb the information and decide. And that may mean you need to think about it for a little while. You might need to get a second opinion. You might need to reach out to resources like AIM that can give you more help maybe in a different way of presenting information. So, take advantage of all those things. There doesn’t need to be a rush around the time of a diagnosis of melanoma.
Fertility and family planning

Dr. Geoffrey Lim: There’s a couple of questions that I wanted to ask you specifically about the patients thinking about fertility and how that affects them, their family planning. Are there any consequences of drug treatment on family planning? How do you have that discussion around adjuvant therapy?
Dr. Jason Luke: Yeah, this is a great question. And it comes up in melanoma more often than in some other kinds of cancers because, unfortunately, some of our patients are younger. The answer for surgery, is that it really does not typically affect family planning. But when we’re talking about medicine, drug therapy for reduction of recurrence after surgery that’s going to go on for a year, then we do really need to be cognizant of this question because in reality, we just don’t know the answer. There is not strong evidence that would say that if you are taking these immunotherapy medicines that you will have a problem with a pregnancy, but at the same time, it hasn’t been thoroughly studied. So, in all of the clinical trials, patients were asked to take approaches that would keep them from getting pregnant.
If fertility and family planning are at all a concern, then absolutely having a discussion with a fertility specialist and potential egg banking is a great idea. And often there’s a fear factor of, “Oh my gosh, I was diagnosed, we don’t have time to think about family planning.” But what we have to reassure and emphasize for people, especially younger patients with melanoma, is we’re thinking about your future over the next fifty, sixty, seventy years. Addressing the melanoma is not just an issue that affects the next two months. We want to make all the decisions that are going to make your life go well, which hopefully is not having melanoma, but that should not come at the expense of the other aspects of life, which obviously are so important. So that’s definitely somewhere where we want to make sure we’re not going too fast and we’re taking into account those kinds of longer-term considerations for quality of life that people might have.
Dr. Geoffrey Lim: That’s an interesting point about not rushing the decision-making process about adjuvant therapy. You’ve mentioned this multiple times. How much time do patients actually have after the final surgery (excision) before adjuvant therapy has to be started?
Dr. Jason Luke: The pembrolizumab trial arbitrarily defined three months as the time frame within which to start adjuvant therapy after the final surgical excision. That’s the time frame used in other adjuvant therapy trials in melanoma. There’s actually no biological reason why that’s the time frame. From the conversations I have had, most people feel pretty comfortable about that three-month time frame, but we do have some cases where we went out to a six-month time frame, especially when pembrolizumab first became available. This was relevant to people who had their surgeries prior to the approval and still wanted to take advantage of the adjuvant therapy option. I can’t speak to whether waiting past the three-month period causes any hiccups with insurance. Beyond six months, we really don’t have any experience, and it’s not clear how much of a benefit you would get at that point. Some experts feel that if you wait too long to start adjuvant therapy, you may just as well wait and treat if the disease comes back. Again, we do not know if adjuvant therapy provides a survival advantage vs waiting to treat the disease when it comes back.
So there is some time to think through the decision and address issues such as family planning. Of course, we can add additional time for decision-making by obtaining the medical oncology referral early—when the pathology results come back from the biopsy. This is also an option. Some groups are now conducting multidisciplinary tumor board discussions with the dermatologist, surgeon, and medical oncologist meeting after the biopsy results are in for patients with Stage II disease. Such tumor boards make sense to make sure the care is coordinated more seamlessly, but an additional benefit is that they also give us more time to establish a relationship between the medical oncologist and the patient and facilitate shared decision making.
Suggested Reading
Luke JJ, Rutkowski P, Queirolo P, et al. Pembrolizumab versus placebo as adjuvant therapy in completely resected stage IIB or IIC melanoma (KEYNOTE-716): a randomised, double-blind, phase 3 trial. Lancet. 2022;399(10336):1718-1729. doi:10.1016/S0140-6736(22)00562-1
Copyright ©2023- - The Melanoma Nursing Initiative. All rights reserved.