Is it true that Stage II melanoma can have a worse prognosis than Stage III melanoma?

Dr. Jason Luke: I think as patients become more aware of information around their melanoma diagnosis and read more about it, they come to this realization that some Stage II melanomas fare worse than certain Stage III melanomas, which seems paradoxical. It can be very confusing. Historically, we thought of high-risk melanoma as being melanoma that involved lymph nodes. And the reason for that was related to our surgical paradigm: we would cut the melanoma off the skin and then we’d check the lymph nodes because that’s the most likely place for melanoma to go first. If melanoma was in the lymph nodes already, well, that meant that it was already spreading and was on its way to spreading to distant sites, so, therefore, that was bad.
It turns out, however, with more long-term data, we observe that for some of the patients who have deep primary lesions without lymph node involvement, the Stage IIB and Stage IIC patients, the outcomes are as bad, possibly worse than for Stage IIIA or IIIB patients who have limited lymph node involvement combined with relatively lower risk primary melanomas, as defined by thickness and ulceration. These results are shown in the Graphic.
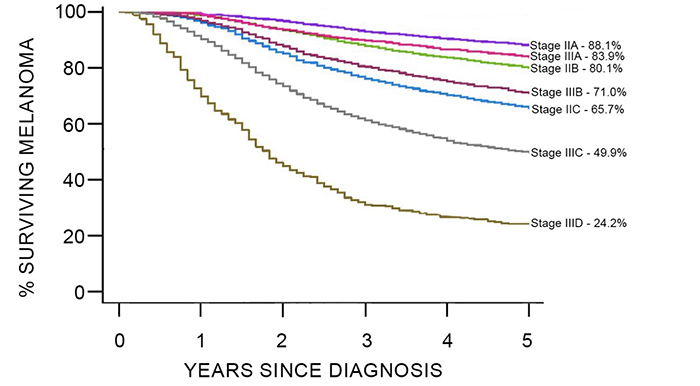
Graphic. Differences in survival time after diagnosis between substages of Stage II and Stage III melanomas. To learn more about these data click here.
And so, then you say to yourself, well wait a minute, maybe lymph node involvement is not always an indicator for high risk for distant metastatic disease. And, now that we have better follow-up on thousands and thousands of people, the biology of melanoma is becoming more obvious to us, which is to say the higher risk the melanoma on the skin (defined by depth and ulceration), the worse situation you have. The characteristics of that primary melanoma are an important driver of outcomes, even in patients who have regional disease.
Summary
Melanoma can be a systemic disease; there is a chance that it can come back even after the primary melanoma has been removed surgically.
Suggested Reading
Bleicher J, Swords DS, Mali ME, et al. Recurrence patterns in patients with Stage II melanoma: The evolving role of routine imaging for surveillance. J Surg Oncol. 2020;122(8), 1770-1777. doi:10.1002/jso.26214
Yang CQ, Wang H, Liu Z, et al. Integrating additional factors into the TNM staging for cutaneous melanoma by machine learning. PloS One. 2021; 16(9):e0257949. doi:10.1371/journal.pone.0257949